The primary aim of this project was to quantify the impact of increasing resistance (either owing to vaccination or to previous infections) as the COVID-19 pandemic evolved. In particular, we addressed the question: “What is the impact of mobility-restricting measures on a resistant population?” In this work we considered two factors: different types of points of interest (POIs)—including transit stations, groceries and pharmacies, retail and recreation, workplaces, and parks—and the emergence of the Delta variant. We studied a group of 14 countries and estimated COVID-19 transmission based on the type of POI, the fraction of population resistance, and the presence of the Delta variant using a Pearson correlation between mobility and the growth rate of cases.
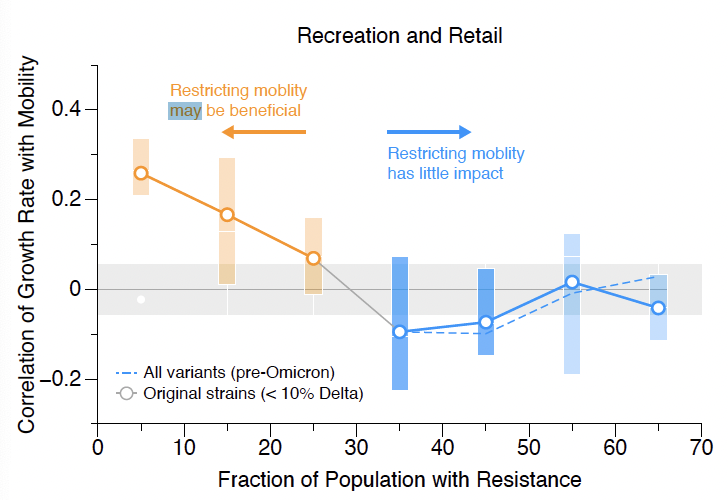
As expected, we found that the effectiveness of mobility-restricting measures decreases as the population becomes more resistant to the virus. This is easily understood by considering two extremes: (1) if the population has perfect resistance, the virus cannot spread at all and mobility-restricting measures have no impact versus (2) a population with no resistance in which, in the absence of isolation, the virus can spread like wildfire. Between these two regimes, lies the interesting policy question namely, “What is the critical fraction of resistance in the population above which there is little benefit to restricting mobility?” The answer to that question depends on the POI in question. We find that retail and recreation venues, transit stations, and workplaces are the POIs that benefit the most from mobility restrictions, particularly if the fraction of the population with resistance is below 25–30%. Groceries and pharmacies may benefit from mobility restrictions when the population resistance fraction is low, whereas in parks, there is little advantage to mobility-restricting measures. These results are consistent for both the original strain and the Delta variant; Omicron data were not included in this work.